En cours Initiatives
Virtual BETTER

The Virtual BETTER Study
The BETTER program has shown the efficacy of using personally tailored one-on-one, in-person prevention visits to increase patients’ chronic disease prevention and screening practices. Given the recent events of the COVID-19 pandemic, however, the use of virtually-delivered healthcare services has been on the rise. While essential in ensuring that some services can still be delivered to patients, little is known about how virtual delivery affects patients’ health outcomes and how populations with limited access to technology, in particular, are impacted.
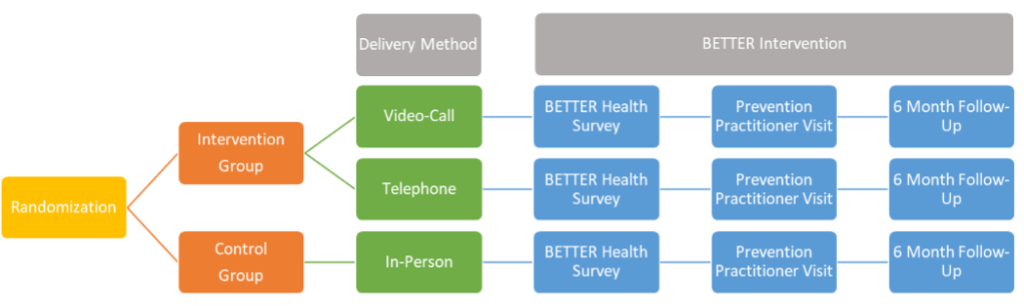
The Virtual BETTER study, which will be based out of Newfoundland and Labrador, will test the BETTER approach delivered via video-call, telephone, or in-person. We will compare things like how many patients agree to participate in a prevention visit by video-call, by telephone, or in-person, whether they were able to connect for the visit successfully, and how they rated their satisfaction with the visit and the quality of the communication with the provider. This information will be used to inform current plans to deliver BETTER and other programs using video and phone. We will also use it to plan for a larger and longer study to compare patients’ behaviour change and uptake of disease screening tests when these different communication methods are used. The results of this study will help shift the focus of the health system towards disease prevention rather than treatment and will help increase accessibility to healthcare.
The Virtual BETTER study will ask the following questions:
- Do patients report similar readiness to implement lifestyle changes after video-call, telephone, and in-person BETTER Prevention visits? Are there factors such as sex, gender, age, or socio-economic status that affect this association?Are there differences between accessibility and acceptability of the different types of visit?
- Are there differences between accessibility and acceptability of the different types of visit?
- Are there differences in satisfaction and the rating of communication issues between patients randomized to the different visit types? Are there factors that affect this association?
- Are the proposed recruitment, randomization, and data collection methods feasible and sufficient to complete a larger trial within the constraints of available funding opportunities?